On April 25, 2011, the NRC dispatched a Special Inspection Team (SIT) to the Perry nuclear plant in Ohio in response to an event three days earlier involving radiation exposure to workers performing maintenance. None of the workers received a radiation dose exceeding federal limits. But the NRC’s SIT found that this outcome was due more to luck than to skill.The boiling water reactor (BWR) at Perry has four movable detectors called Source Range Monitors (SRMs) that monitor the reactor’s power as it is starting up. The SRM are only intended to be used at low power levels – up to about one percent of rated power. An SRM detector is about one inch long and about 0.16 inches in diameter. The detectors are attached to cables that are nearly 40 feet long. The detectors and their cables are located within hollow metal tubes that rise vertically from the domed bottom of the reactor vessel. Electric motors beneath the reactor vessel allow the SRMs to be inserted to a position 18 inches above the mid-point of the reactor core when the reactor is shut down or operating at very low power levels. Once the Intermediate Range Monitors (IRMs) have been demonstrated to be tracking power level during startups, the SRMs are withdrawn to a position 2 ½ feet below the bottom of the reactor core. Figure 1 provides a side view of a reactor vessel indicating the reactor core location and the SRM travel range.
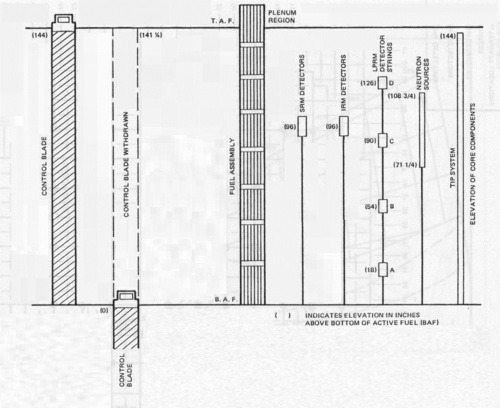 Figure 1.
Figure 1.
Workers replaced SRM detector C in February 2009. SRMs are replaced periodically when their sensitivities decrease due to consumption of the material inside the detectors or wear and tear of their cables. During a reactor startup in May 2010, the operators were unable to retract SRM C from the reactor core. Remaining in the reactor core during high power operation quickly disabled SRM C. It was scheduled to be replaced at the next refueling outage.
Operators shut down the reactor on April 18, 2011, for refueling. On April 22, 2011, workers entered the area beneath the reactor vessel to remove SRM C and replace it. Figure 2 shows the undervessel area at Perry. Their assignment was to cut the cable for SRM C and attach the cut end to a spool in a portable tape-up cartridge they carried into the area. Figure 3 shows the actual take-up cartridge used at Perry. The workers would then exit the undervessel area and remotely turn the cartridge’s spool to pull the cable and SRM C into the cartridge. The cartridge would then be placed in a lead cask for shielding against the high levels of radiation being emitted. (The plant’s owner calculated that the radiation levels one inch from the SRM detector were 66 rem per second, yielding a lethal exposure in about 7 seconds – hence the remote handling provisions.)
 Figure 2.
Figure 2.
 Figure 3.
Figure 3.
While many problems factored into this event, the primary problem was length. The take-up cartridge was designed to hold 30 feet of cable and the detector. But the cable for SRM C was 39 feet long. To work around this design shortcoming, workers had to cut the SRM’s cable twice. They would cut the cable, pull the SRM down 9 feet, then cut the cable again. They would attached the shortened cable to the spool in the take-up cartridge and remotely retract the cable and detector.
The written procedure guiding the workers on April 22nd instructed them to cut the cable “when radiation level raises and/or there is approximately 30’ of cable left” in the tube. The cable isn’t marked like a measuring tape with periodic readouts indicating 37 feet left, 36 feet left, and so on. Instead of pulling the SRM detector 9 feet out, the workers pulled nearly 22 feet of cable from the tube. In doing so, they pulled the very hot SRM detector much closer to them. The radiation levels in the undervessel area skyrocketed from about 2 rem per hour to over 1,000 rem per hour (the actual radiation levels are unkown – the instrumentation being used did not record valves above 1,000 rem per hour and pegged at the highest value they could indicate.)
Two radiation protection specialists were present at the job site. One specialist was in the undervessel area with the workers. The second specialist was located just outside the area monitoring telemetered radiation readings from the individual workers and other locations in the area. When these radiation protection specialists advised the workers about the extremely high radiation levels, the workers exited the area extremely fast. The electronic dosimeters worn by the workers revealed the maximum exposure was 0.098 rem, far below the federal limit of 5 rem per year for nuclear workers.
The NRC’s SIT found many faults with the radiation protection provided to these workers, including:
- The radiation protection instructions for this replacement of SRM C were copied from the instructions applied to the replacement of IRM C during a refueling outage in 2005 without accounting for the significantly higher radiation levels resulting from SRM C having resided inside the core of an operating reactor for nearly one year.
- The instrumentation used to monitor radiation during the work was not sufficient to monitor the range of potential radiation levels.
- The guidance provided to the workers was not sufficient to prevent excessive cable from being removed.
- The radiation protection specialists wore headsets to enhance communications between themselves, but none of the workers had access to that communications channel.
- The work area had many traps, like open grating for workers to fall through and tripping hazards across the grating (see Figure 4), that could have delayed workers exiting the area before receiving radiation exposures exceeding federal limits.
 Figure 4.
Figure 4.
The NRC’s SIT report identified one potential white and one green finding related to violations of federal regulations.
Our Takeaway
These workers at Perry were set up and fortunately avoided paying a higher price. The take-up cartridge serves only one purpose – to hold the cable and detector of an in-core instrument being replaced. It’s inexcusable to use a cartridge too small to perform that single purpose, forcing workers to take risky steps to make it work. The procedure directed the workers to remove the cable until 30 feet remained inside its tube – an illogical direction. The work plan contained few measures to protect the workers when things went wrong – such as conducting the work with many impediments to a rapid exit.
Despite the shortcomings, some things worked. The radiation protection specialists got the workers out of the danger zone before they received radiation exposures above federal limits. And even though none of the workers’ exposures exceeded federal limits, the NRC dispatched a special inspection team to determine why this near-miss occurred.
It’s unfortunate that avoidable events happen. But the silver lining is when, as in this case, such events are taken seriously and their lessons are heeded so as to make repeat events even easier to avoid.
“Fission Stories” is a weekly feature by Dave Lochbaum. For more information on nuclear power safety, see the nuclear safety section of UCS’s website and our interactive map, the Nuclear Power Information Tracker.